 +91 63713 07504
+91 63713 07504
What is TAVI in Cardiology?
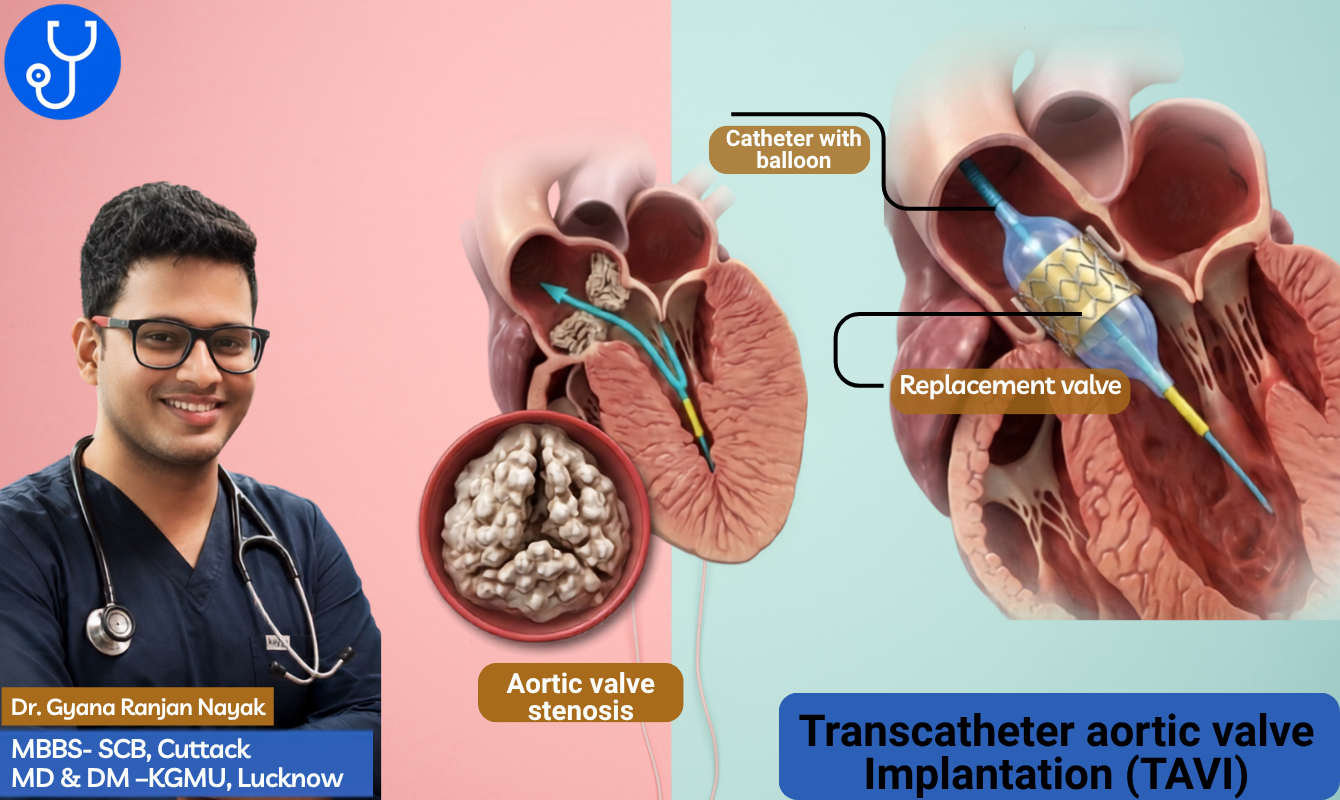
TAVI, or transcatheter aortic valve implantation, aka TAVR (transcatheter aortic valve implantation) is a minimally invasive procedure which a diseased aortic valve without opening the chest. It is mainly used to treat severe aortic stenosis, a condition in which the valve becomes narrowed and makes it harder for the heart to pump blood.
Unlike open-heart surgery that usually involves a large surgical incision and bypass surgery, TAVI involves less pain, shorter hospital stays, and faster recovery.
For many patients with severe aortic stenosis, especially those who are older or at higher surgical risk, TAVI can be a safer and less invasive treatment option.
In this guide, I have explained what TAVR is, how it works, the right candidates, risks, post-operative care, and many more valuable information. Please keep reading and I hope this information can help you or your loved ones.
Why TAVI is Considered a Better Option than Open-Heart Surgery?
TAVI is considered a strong alternative to open-heart surgery because randomized trials in selected patients have shown similar major outcomes, with the advantage of being less invasive. In low-risk patients, the PARTNER 3 trial reported that SAPIEN 3 TAVI was superior on the composite endpoint of death, stroke, or rehospitalization at 1 year, and the 5-year Evolut Low Risk trial showed similar rates of death or disabling stroke between TAVI and surgery, with 15.5% vs 16.4% respectively.
That evidence is why the 2020 ACC/AHA Valvular Heart Disease guideline includes transfemoral TAVI as a Class I option for symptomatic patients aged 65 to 80, and prefers it in patients older than 80 or in those with high or prohibitive surgical risk when expected survival and quality of life are acceptable.
In Europe, the ESC/EACTS valvular heart disease guidance also uses randomized trial evidence and registry data to support TAVI in appropriately selected patients, rather than treating it as a universal replacement for surgery.
Important: Although TAVI is a proven option for many patients, it is not automatically better for everyone. People at high surgical risk, low surgical risk, or with specific valve anatomy still need an individualized evaluation before any treatment decision is made.
How the TAVI procedure works?
TAVI is typically performed through a small incision in the groin, though other access routes may be used in selected patients. The catheter carries the replacement valve to the heart, where it is expanded inside the diseased valve and starts working immediately.
The procedure usually takes about 1 to 1.5 hours in patient information from FDA-linked material on a TAVI valve system. After the valve is placed, the catheter is removed and the small access site is closed.
Typical steps
- The patient is evaluated by a heart team and undergoes imaging such as echocardiography.
- The procedure is done under anesthesia or sedation, depending on the center and patient profile.
- The new valve is delivered through a catheter and positioned inside the old valve.
- The heart valve begins functioning immediately, and the patient is monitored for recovery.
TAVI vs. Open Surgery
TAVI or TAVR is not the same as traditional open-heart valve replacement, which is also called SAVR. In open heart surgery, the surgeon open the chest, temporarily stopping the heart, while TAVR skips that large surgical incision.
According to standard guidelines, SAVR is recommended for patients younger than 65 with longer life expectancy, while TAVI is favoured more often in older patients or those with higher surgical risk. For patients aged 65 to 80, the choice is usually based on anatomy, risk, and shared decision-making.
TAVI vs. Open Heart Surgery- A Comparison
| Factor | TAVI | SAVR |
|---|---|---|
| Chest opening | No | Yes |
| Recovery | Usually faster | Usually longer |
| Typical candidates | Older or higher-risk patients, and selected lower-risk patients | Younger patients, certain anatomies, or when durability is prioritized |
| Hospital stay | Often same day to next day, depending on center | Usually longer |
| Main tradeoff | Less invasive, but durability and pacemaker issues matter | More invasive, but long-term durability is well established |
Benefits of TAVR
Patients often choose TAVI because it is less invasive and usually involves a shorter hospital stay and faster return to daily activities. Many patients go home the day of the procedure or the next day.
Other benefits include less pain than open surgery, faster mobility, and improvement in symptoms such as breathlessness and fatigue. Data from the FDA Summary of Safety and Effectiveness Data (SSED) demonstrates that TAVR significantly reduces mortality in patients ineligible for open surgery.
Risks and limitations
While TAVR is a life-changing alternative to open-heart surgery, the Food and Drug Administration (FDA) emphasizes that it is still a major medical procedure with serious risks. According to official FDA Patient Information Guides, potential complications include stroke, severe bleeding, and damage to the blood vessels used during the procedure.
Furthermore, patients face risks of abnormal heart rhythms, the potential need for a permanent pacemaker, and temporary kidney injury caused by the contrast dye used during imaging.
Long-term valve durability also remains important, especially for younger patients. The FDA Patient Information Booklet for newer transcatheter heart systems explicitly notes that long-term clinical durability has not yet been fully established.
This unknown lifespan is exactly why medical teams at major institutions like the Cleveland Clinic emphasize that rigorous, routine follow-up care is absolutely essential for tracking valve health over time.
Who is an Ideal Patient for TAVI?
Choosing between a less invasive TAVI procedure and a traditional open-heart surgery comes down to a lot more than just the number on a birthday cake. To determine if someone is an ideal candidate for TAVI, a specialized medical team looks at the big picture of a patient’s overall health, physical build, and daily quality of life.
What Doctors Look at (Beyond Your Age)
Age is just a starting point. To map out the safest path forward, a multidisciplinary heart valve team evaluates several crucial health factors:
- Valve Disease Severity: Confirming how narrow the aortic valve has become and if it is actively causing symptoms like extreme fatigue or breathing issues.
- Open Surgery Risk: Calculating how risky a traditional open-chest procedure would be based on a patient’s baseline health.
- Your Unique Anatomy: Mapping out the precise shape of the heart valve and measuring the size of blood vessels to ensure a catheter can pass through safely.
- Organ Health: Checking kidney function to verify the body can safely process and clear the contrast dye used during the imaging phase.
- Meaningful Recovery: Ensuring the procedure will actually help the patient get back to enjoying life, rather than just extending a painful recovery timeline.
The Official Age Guide (According to Heart Experts)
The American College of Cardiology (ACC) and American Heart Association (AHA) publish joint guidelines to help doctors break down treatment paths by age bracket:
Under 65 Years Old
Traditional Surgical Aortic Valve Replacement (SAVR) is usually the top choice.
Younger patients generally have a long life expectancy ahead of them. Because surgical heart valves traditionally have a longer track record of durability, SAVR helps delay the need for risky follow-up operations decades down the road.
Ages 65 to 80
Both TAVI and SAVR are on the table.
This is a grey area where the choice comes down to personal anatomy and a process called shared decision-making.
The patient and the ACC Heart Valve Team sit down together to weigh out personal preferences, recovery goals, and physical health.
Over 80 Years Old (or High Surgical Risk)
TAVI is almost always the preferred path.
For older adults or individuals who are too fragile to handle open-chest surgery, TAVI offers a much gentler recovery.
According to clinical insights compiled on the NCBI Bookshelf, TAVI is highly favoured as long as the patient is expected to live for at least 12 more months with a vastly improved quality of life.
Recovery after TAVI
In most cases, Patients can walk within hours, leave the hospital in less than 24 hours, and return to light activities and work within a couple of weeks.
Expected Recovery Timeline
While TAVI has a drastically faster recovery window than traditional open-heart surgery, patients should follow a structured progression.
- 0 to 24 Hours Post-Procedure: Most patients are sitting up within hours and are assisted to walk by the following day. Hospital stays are generally between 1 to 2 days.
- 1 to 2 Weeks Post-Procedure: Patients can often return to work and resume light daily tasks.
- 4 Weeks Post-Procedure: Patients are typically cleared to resume driving, provided there are no complications.
- 6 to 10 Weeks Post-Procedure: Full physical and internal healing is typically achieved.
Post-Operative Care
- Medications: Adhering to antiplatelet or anticoagulant regimens is vital to prevent blood clots on the new valve.
- Wound Care: The incision site (usually in the groin) must be monitored for signs of infection.
- Cardiac Rehabilitation: Your cardiologist may refer you to a structured rehabilitation program within several days of the procedure to safely rebuild strength and endurance.
Success and outcomes
The clinical data regarding TAVR demonstrates highly reassuring success rates. Studies focused on our population in India confirm that the procedure delivers excellent early recovery metrics and robust mid-term survival rates, matching international benchmarks.
Indian Clinical Results
1-Year Mortality Rate: Data tracking TAVR outcomes within Indian healthcare centers indicates a 1-year all-cause mortality rate of approximately 8%. This closely mirrors global safety standards and confirms the efficiency of the overall procedure for our patients.
Stroke Rates: The incidence of a major disabling stroke—meaning a severe stroke that causes permanent, long-term damage like paralysis or loss of speech—remains exceptionally low across Indian centers. Complications, when they do occur, are typically minor, non-disabling, and concentrated within the first week post-procedure, highlighting the importance of focused early monitoring.
The Reintervention Reality: Similar to international findings, long-term tracking shows a slightly higher rate of minor valve adjustments or repeat procedures over time compared to open surgery. However, this trade-off is balanced by the rapid, minimally invasive recovery process.
Addressing the Indian Patient Reality
Bicuspid Valve Anatomy: While major Western trials primarily track standard tricuspid valves, Indian patients frequently require intervention at a younger age, presenting with a much higher percentage of bicuspid aortic valves. Local registry data shows a 98% procedural success rate in these cases, demonstrating that advanced pre-operative CT mapping effectively mitigates the anatomical challenge.
Vessel Diameter Adjustments: Indian patients, particularly women, naturally present with smaller femoral artery diameters compared to Western demographics. To manage vascular risks, our local protocols utilize ultra-low-profile delivery catheters designed to navigate smaller vessels safely.
Pacemaker Requirements: Because bicuspid valves require precise radial force to expand fully, the permanent pacemaker implantation rate sits around 11.4% post-procedure. While this is slightly higher than in tricuspid valves, long-term follow-up from clinical outcome monitoring confirms these patients remain entirely stable with zero secondary complications.
Experienced Centers and Innovation
Hospital Volume Metrics: In transcatheter therapies, institutional volume dictates success. High-volume Indian heart teams that perform this procedure routinely demonstrate immediate success rates between 95% and 98%.
Validation of Local Tech: Patient confidence is further supported by the deployment of contemporary, Indian-manufactured valve systems (such as Meril’s Myval). These platforms have been validated in rigorous clinical trials, showing excellent hemodynamic stability and minimal paravalvular leaks right here in our hospitals.
FAQs
Is TAVR better than open-heart surgery?
Not universally. TAVR or TAVI is less invasive and often easier to recover from, but the best option depends on age, anatomy, and long-term durability needs.
How long does a TAVI valve last?
Valve durability is good, but long-term performance depends on the device and patient profile. Some FDA material still emphasizes the need for ongoing follow-up because durability data for newer systems continue to evolve.
Will I need a pacemaker after TAVI?
Some patients do need one after TAVR, especially with certain valve types or conduction-system changes. This is a known risk and should be discussed before the procedure.
How fast can I walk after TAVI?
Many patient guides say walking begins within hours, and normal activity returns gradually over days to weeks. Exact timing depends on access route, overall health, and whether any complication occurs.
